Why Are My Teeth Sensitive?
One mechanism sits behind nearly every kind of tooth sensitivity. Understand it, and the causes - and the fixes - fall into place.

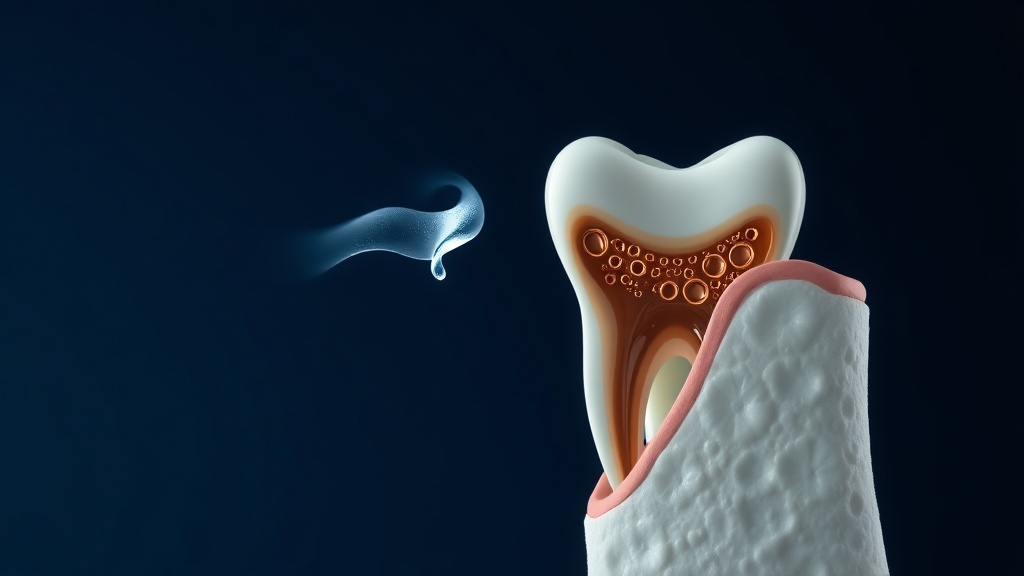
- Almost all tooth sensitivity comes down to one thing: dentin - the softer inner layer threaded with nerve-linked tubules - has become exposed, whether by receding gums or thinning enamel.
- Once dentin is exposed, the hydrodynamic theory explains the pain: cold, heat, sweet, acid or touch move the fluid inside the tubules, and that movement triggers the nerve as a short, sharp zing.
- It is very common. Reviews estimate roughly 15-20% of adults have dentin sensitivity, most often between about 20 and 50 years old, with gum recession the single biggest route to exposed dentin.
- The usual causes are recession, enamel erosion from acid, abrasion from hard brushing, grinding, cracks, whitening, and recent dental work - different doors to the same exposed-dentin problem.
- Relief works on two fronts: plugging the open tubules (stannous fluoride, arginine) and calming the nerve (potassium), plus removing whatever is exposing the dentin in the first place.
Teeth are sensitive when the dentin beneath the enamel and gum becomes exposed, opening tiny fluid-filled tubules that lead to the nerve. Cold, sweet, acid or touch then move that fluid and the nerve reads it as pain. Gum recession, enamel erosion, hard brushing, grinding, cracks and whitening are the common ways dentin gets exposed.
The one mechanism behind nearly every cause
Tooth sensitivity looks like it has many causes, but they nearly all lead to a single place. Your tooth is shielded by enamel on the crown and gum-plus-cementum on the root. Beneath that shield is dentin, and dentin is not solid - it is packed with microscopic tubules full of fluid, each running inward toward the nerve. As long as the shield is intact, the dentin never feels anything. Sensitivity begins the moment the dentin is exposed and its tubules are open at the surface and still connected to the pulp. From there, the hydrodynamic theory takes over: any stimulus that moves the tubule fluid quickly - a cold sip, a sweet bite, an acidic drink, a brush bristle, a blast of air - bends the nerve endings at the far end of the tubules, and the nerve reports it as a fast, sharp pain. This is why such different triggers all produce the same kind of zing, and why the many named causes of sensitivity are really just different ways of arriving at exposed dentin. Understand that, and both the causes and the fixes stop feeling random: expose the dentin and it hurts; cover or calm the dentin and it settles.

Recession, erosion, abrasion, grinding, cracks and whitening are different doors to the same room: exposed dentin.
What the research actually shows
Every claim below maps to a named, peer-reviewed source in the Sources section. According to PubMed.
| Claim | Evidence | Source |
|---|---|---|
| The hydrodynamic theory is the most accepted mechanism of dentinal sensitivity: a stimulus changes fluid flow in the dentin tubules, activating the nerve. | Narrative review of sensitivity mechanisms. | Aminoshariae & Kulild, 2021 |
| Dentin sensitivity is multifactorial, developing when two or more factors combine to cause loss of enamel and/or cementum, and it most affects middle-aged people. | Review of aetiology, prevalence and mechanism. | Al-Sabbagh et al., 2004 |
| Roughly 15-20% of adults are affected, peaking between 30 and 39; gingival recession is the primary cause of dentin exposure. | Review of epidemiology and management. | Cummins, 2009 |
| Enamel begins to dissolve below a critical pH of about 5.5, so dietary acid is a major route to the enamel loss that exposes dentin. | Review of erosive tooth wear and enamel pH. | Lussi et al., 2011 |
| A stannous fluoride toothpaste occluded about 82% of dentin tubules versus 35% for control and significantly reduced sensitivity, one of two main relief strategies. | In-vitro plus double-blind clinical study. | Hines et al., 2019 |
The common causes, and how each exposes dentin
| Cause | How it exposes dentin | Your main lever |
|---|---|---|
| Gum recession | Uncovers the root, which has no enamel | Gentle brushing; occluding paste |
| Acid erosion | Dissolves and thins the enamel surface | Cut acid; support remineralization |
| Hard brushing (abrasion) | Wears enamel and gum at the gumline | Soft brush, light pressure |
| Grinding and clenching | Flexes teeth and chips enamel edges | Night guard; desensitizing paste |
| Cracks and worn fillings | Opens a direct path to the dentin | See a dentist to repair |
| Whitening | Briefly opens tubules and irritates the pulp | Desensitizing paste; usually temporary |
Why relief comes in two flavors
Because sensitivity is a plumbing problem, the proven relief tools work on the plumbing in two different ways, and knowing which is which makes choosing a product far less confusing. The first approach plugs the tubules so stimuli cannot move the fluid inside. Stannous fluoride deposits a mineral coating that seals the openings, and in testing it plugged the large majority of tubules while a plain paste barely did. Arginine with calcium carbonate builds a calcium-phosphate plug that resists the normal pressure inside a tooth. The second approach leaves the tubules alone and calms the nerve directly: potassium salts surround the nerve endings and make them less able to fire, turning the signal down. Both are genuine, and both take a few weeks of consistent use rather than working instantly - the evidence for potassium in particular is real but modest. Sitting underneath both is a third, easily forgotten step: removing whatever is exposing the dentin in the first place. Switching to a soft brush, easing off acids, wearing a night guard for grinding, or having a crack repaired all stop new dentin from being exposed. The most reliable results come from combining a desensitizing paste with fixing the underlying cause, rather than relying on toothpaste to outrun a habit that keeps stripping the shield away.
Evidence you can act on.
Occasional emails — new research, new protocols, no noise.
A general approach to sensitive teeth
This works for most exposed-dentin sensitivity. It calms the nerve, seals the tubules, and removes common causes. It does not repair cracks, cavities or failing fillings - those need a dentist. Give it two to four weeks.
- 1
Start a desensitizing toothpaste
twice dailyChoose one that plugs the tubules (stannous fluoride or arginine with calcium carbonate) or calms the nerve (potassium nitrate). Use it morning and night, and let the benefit build over several weeks rather than expecting an overnight change.
- 2
Leave a little on the sensitive areas
nightlyAfter brushing, rub a small amount onto the tender spots and leave it rather than rinsing everything away. Extra contact time gives the plugging or calming ingredients more chance to work.
- 3
Switch to a soft brush and lighten your touch
every brushingHard, scrubbing brushing is a leading cause of the recession and enamel wear behind sensitivity. A soft brush and gentle, short strokes protect the shield you still have.
- 4
Ease off acids and time your brushing
dailyAcidic drinks and foods soften enamel; rinse with water after them and wait 30 to 60 minutes before brushing. Keeping the surface above its critical pH protects against the erosion that exposes new dentin.
- 5
Address grinding and get cracks checked
as neededIf you clench or grind, a night guard reduces the flexing that chips enamel. And if one tooth is sharply painful or sensitive from a specific spot, have a dentist check for a crack or cavity rather than relying on paste.

Relief comes in two flavors - plug the tubules or calm the nerve - and works best alongside removing the cause.
Everyday sensitivity is a brief zing that fades with the trigger. See a dentist if pain comes from one specific tooth, lingers or throbs, arrives on its own, hurts when you bite down, or is joined by swelling, a bad taste, or visible discoloration. Those patterns can mean a cavity, a cracked tooth, a failing filling, gum disease, or an inflamed pulp - problems that need diagnosis and repair. A desensitizing routine calms exposed dentin, but it cannot fix broken tooth structure, so lasting or localized pain should always be examined in person.
Frequently asked questions
Sources
- 1.
- 2.
- 3.
- 4.
- 5.
- 6.

Fix your breath at the source.
The complete science-backed protocol — engineered to eliminate volatile sulfur compounds at the biological source.
Start the Breath Protocol →Related reading
Educational purposes only. The content on this page is not medical advice and is not a substitute for consultation with a qualified dental or medical professional.
More from the library
 Causes8 min
Causes8 minWhy Are My Teeth Sensitive to Cold? The Real Reason (and What Helps)
A cold sip should not sting. Here is why it does, and the two proven ways to quiet it.
Read →→ Causes8 min
Causes8 minWhy Do My Teeth Hurt When I Eat Sweets? The Osmotic Trigger Explained
Sweetness itself is not painful. Here is why sugar makes an exposed tooth zing, and the one pattern you should never ignore.
Read →→ Causes8 min
Causes8 minSudden Tooth Sensitivity: Why It Started and When to See a Dentist
When sensitivity arrives suddenly, the timing is the clue. Here is how to read it - and the signs that mean call a dentist now.
Read →→ Answers9 min
Answers9 minHow to Get Rid of Sensitive Teeth: An Evidence-Based Relief Routine
The relief that works is simple, but the details matter. Here is the routine, ingredient by ingredient.
Read →→ Answers8 min
Answers8 minHow to Get Rid of White Spots on Teeth: Your Options, Ranked
An honest, evidence-based ladder of options, from what you can do at home to what only a dentist can fix.
Read →→ Ingredients8 min
Ingredients8 minHydroxyapatite Toothpaste Benefits: What the Evidence Actually Supports
A calm, science-first look at what hydroxyapatite toothpaste can genuinely do for your enamel, and where the evidence stops.
Read →→