Gum Recession: A Complete Guide to What's Happening and What Actually Helps
A clear, evidence-based map of gum recession — what it is, what drives it, and the honest truth about what you can and cannot change at home.

- Gum recession is when the gum margin moves — or is worn — back from the tooth, exposing part of the root that enamel never covered. It is extremely common, affecting most adults on at least one tooth.
- The most important honest truth: gum tissue that has already receded does not grow back on its own. No paste, rinse, oil, gel, or brushing routine regrows lost gum — only surgery by a periodontist can cover an exposed root.
- What good home care CAN do is real and worth doing — it can slow or stop recession from getting worse by removing its two main drivers, plaque and brushing trauma.
- Recession has two overlapping cause families: mechanical wear (hard or abrasive brushing) that favours the cheek-side surfaces, and inflammatory gum disease that destroys the supporting attachment from below.
- Because recession is progressive and cannot be reversed at home, the win is early: catch it, remove the cause, and get a professional assessment before more root is exposed.
Gum recession is when the gum edge moves back and exposes part of the tooth root. It is usually driven by too-hard brushing, plaque-related gum disease, or both. Receded tissue does not grow back on its own — but removing the cause can stop it worsening, and a periodontist can surgically cover exposed roots.
What gum recession actually is
Your teeth are covered by hard enamel only down to a line near the gum called the cementoenamel junction. Below that line the root is covered not by enamel but by a thin layer of cementum, and it is meant to sit tucked safely under the gum. Gum recession is simply the gum margin moving — or being worn — back past that line, so a strip of root is left exposed. Because that exposed surface is softer and threaded with microscopic tubules leading toward the nerve, the first thing most people notice is a jolt of cold sensitivity, or a tooth that suddenly looks longer than its neighbours. Recession is not a single disease with a single cause, and the pattern gives it away: it is consistently more common and more severe on the buccal, cheek-facing surfaces than on the surfaces between the teeth. That distribution is the fingerprint of mechanical wear and abrasion rather than infection alone, which is why the story of your gums is often as much about how you brush as about the bacteria in your mouth.
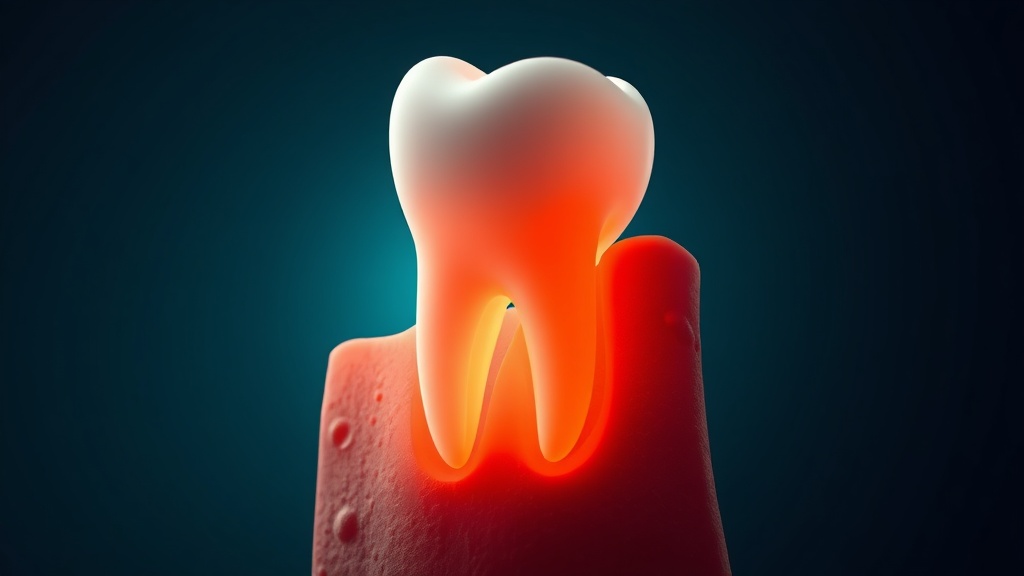
Recession exposes the softer root surface below the enamel line — which is why the first sign is often cold sensitivity or a longer-looking tooth.
What the research actually shows
Every claim below maps to a named, peer-reviewed source in the Sources section. According to PubMed.
| Claim | Evidence | Source |
|---|---|---|
| About 22.5% of US adults aged 30 and over have 3 mm or more of recession on at least one tooth surface, and recession is consistently more common and severe on the cheek-side surfaces. | NHANES III national survey. | Albandar & Kingman, 1999 |
| Across seven European countries, 87.9% of adults had at least 1 mm of recession on one or more teeth — it is close to universal with age. | Multi-country study (n=3,551). | West et al., 2024 |
| Gingivitis (plaque inflammation) is reversible with good plaque control, but the attachment loss of periodontitis is irreversible. | EFP consensus report. | Chapple et al., 2015 |
| The only spontaneous re-coverage of an exposed root in the literature (creeping attachment) occurs only after gum surgery, and even then is incomplete and unpredictable. | Literature review. | Wan et al., 2020 |
| Left untreated, recession sites drifted a further 0.7–1.0 mm apically over 10–27 years, while grafted sites gained and held coverage. | Long-term split-mouth study. | Agudio et al., 2009 |
What drives recession — and what you can change
| Driver | What it does to the gum | Can home care change it? |
|---|---|---|
| Too-hard or abrasive brushing | Mechanically wears the thin cheek-side gum back | Yes — switch to a soft brush and a gentle technique |
| Plaque and gum inflammation (gingivitis) | Swells and breaks down the gum margin | Yes — daily plaque control reverses gingivitis |
| Periodontitis (attachment and bone loss) | Permanently destroys the support beneath the gum | Partly — you can arrest it, not reverse it |
| Thin gum type or tooth position | Less tissue to begin with, more easily triggered | No — it is anatomy; manage the other drivers |
| Smoking | Raises recession risk and blunts healing | Yes — quitting lowers risk over time |
Why receded gums don't grow back — and what that means
Here is the part the internet most often gets wrong. Once the gum has receded, the attachment that held it — the fibres, the cementum, and the underlying bone — is gone, and the body does not spontaneously rebuild that scaffold over an exposed root. Reviewers who have searched the whole literature find only one form of spontaneous re-coverage, called creeping attachment, and it appears only after mucogingival surgery has already been performed — and even then it is partial and unpredictable. In plain terms: no paste, rinse, oil, gel, or brushing routine regrows lost gum. The only way to actually cover an exposed root is periodontal plastic surgery, in which a periodontist moves or grafts tissue over it. That can sound bleak, but it carries a genuinely hopeful flip side. While you cannot get the tissue back at home, you have real power over whether you lose more. Recession is progressive: untreated sites tend to creep further year after year, so removing the cause is the entire difference between gums that stay stable and gums that keep slipping.
Evidence you can act on.
Occasional emails — new research, new protocols, no noise.
How to stop recession getting worse
You cannot regrow the tissue at home, but you can remove the forces driving it back so the recession stops advancing. None of this treats a disease — it protects the gum you still have.
- 1
Switch to a soft brush and ease off the pressure
every brushForce, not plaque, is what physically wears the cheek-side gum away. Use a soft-bristled brush, hold it like a pencil rather than a fist, and let the bristles do the work at a gentle 45-degree angle. Powered brushes reduce plaque and gum inflammation modestly, and a pressure sensor helps habitual scrubbers unlearn the force.
- 2
Clean between the teeth gently, every day
once dailyPlaque left along and between the gumline keeps the margin inflamed. Interdental brushes sized to your gaps, or a low-pressure water flosser, clear it without the abrasion of sawing floss. Keep it gentle — the goal is clean, not scrubbed.
- 3
Protect the margin from your own habits
ongoingIf you grind or clench, ask about a nightguard; if you have a lip or tongue piercing rubbing a gum, consider removing it. These local stresses quietly drive recession at the exact spot they touch.
- 4
Remove the big multipliers
ongoingSmoking raises recession risk and slows healing, so a quit plan is one of the highest-value moves you can make. Support your gum collagen with adequate vitamin C from everyday food — it is a genuine cofactor for building collagen, though eating collagen itself has no gum evidence.
- 5
Get a professional baseline
one visitAsk a dentist or periodontist to measure your recession and the attachment between your teeth so change can be tracked, and to tell you whether a graft is worth considering for any exposed root.

Gentle, low-pressure brushing with a soft brush is the single biggest lever most people have to stop recession advancing.
Any recession that is visibly getting worse, exposing more root, or coming with bleeding, swelling, deep pockets, or loose teeth should be assessed in person — promptly. Only a dentist or periodontist can tell whether you are dealing with mechanical wear, active gum disease, or both, and only surgery can cover an exposed root. Seeing a professional early is what keeps a manageable single site from becoming widespread loss. This article is educational and is not a diagnosis.
Frequently asked questions
Sources
- 1.
- 2.
- 3.
- 4.
- 5.
- 6.
- 7.
- 8.
- 9.

Fix your breath at the source.
The complete science-backed protocol — engineered to eliminate volatile sulfur compounds at the biological source.
Start the Breath Protocol →Related reading
Educational purposes only. The content on this page is not medical advice and is not a substitute for consultation with a qualified dental or medical professional.
More from the library
 Guides8 min
Guides8 minGum Recession Treatment: Every Option, Compared
The right treatment depends on why your gums receded and how far. Here is the full ladder, with what each rung can honestly deliver.
Read →→ Guides8 min
Guides8 minHow to Stop Receding Gums: What Actually Slows It
You cannot will your gum line back up, but you can often stop it from dropping further. Here is what the evidence supports.
Read →→ Answers8 min
Answers8 minCan Receding Gums Grow Back? The Honest Answer
It is the question everyone with recession asks. The straight answer, and what you can realistically do instead.
Read →→ Causes8 min
Causes8 minWhy Are My Gums Receding? The Real Causes
A personal walk-through of why gums recede, how to spot which cause is driving yours, and what to do about each one.
Read →→ Guides8 min
Guides8 minGum Disease Symptoms: The Early Warnings You Can Feel
The symptoms of gum disease you can feel and notice yourself, why bleeding comes first, and when a symptom means see a dentist now.
Read →→ Guides8 min
Guides8 minPeriodontal Disease: The Full Spectrum, Explained
A clear, honest overview of periodontal disease as a spectrum: the difference between gingivitis and periodontitis, what the colloquial phrase gum disease misses, and why early bleeding is the signal to act.
Read →→